deaddebate
Moderator
-
Joined
-
Last visited
Everything posted by deaddebate
-
Deployment waivers should be fairly fully evaluated for real consideration by the gaining location. If the clinic can't resolve the lab results, submitting an incomplete waiver may be their only option. The Flight Doc could still recommend deployment and your SGH can be a good advocate. If you hear that they are submitting a deployment waiver request, I recommend you attempt to talk to the SGH to plead your case so s/he is on your side. If you can go see the Hematologist, that could be your best bet for a stronger waiver or perhaps a definitive diagnosis, however the referral process independently can take weeks due to the current workload of all the VSP/TERA/Non-Vol cases working through the MTF's/TriCare. Talk to your TriCare referral rep. If you don't deploy, it doesn't force an MEB, it just flags you for review and consideration. This usually means an MEB, but in your case, it sounds like you just need time to get properly diagnosed/treated. Hopefully your most recent CBC is normal and this is just a hiccup in your processing.
-
You apparently don't know the extent to the bureaucracy in the MDG. Medical Hold is less common and more difficult than it once was, but it still happens to to at least one patient at every MTF every year. Last year, we had 6 cases that were considered for Medical Hold, 2 actually ended up staying beyond their original DOS. Enlisted have the option to waive the MEB/Med Hold--it's more complicated for Officers. Much is dependent on the condition and amount of evaluation already completed. In one unique case, I saw an M-RILO (Modified Review In Lieu Of Medical Evaluation Board) initiated, submitted, and adjudicated in one day. Very rare, but the condition was only for mild-mod sleep apnea. This is why I've posted multiple times that if you have a condition that might go to MEB, you should have reported it immediately, but if that accidentally slipped your mind, you ought to begin the evaluation 12-24 months before your DOS/DOR, NOT <30 days.
-
Could you be more specific? Also, getting a deployment cancelled highlights you for MEB consideration, which could be much longer than the deployment.
-
It is very likely due to the recent elevation change. Most likely, your doc will order another hemoglobin/hematocrit lab in 3 months or so, and it should be normal. If abnormal, you'll likely be referred to a Hematologist for possible polycythemia. If you are indeed diagnosed with polycythemia, you would be considered for a waiver under the Thrombocytosis umbrella of conditions, in which waiver is almost a certainty. Realistically, this isn't something to worry about. At worst you'll get a waiver in 6-12 months. At best, you won't even get a temp DNIF and just repeat labs once a year until it stabilizes.
-
Depends on the specifics of your DQ waiver and your remaining or new ADSC. Are you DQ'd from ALL flying classes or just FCI/II? What about UAV/GBC? Regardless, re-assignment ownership would likely flow back to AFPC Assignments. I've seen this for several Enlisted but Officer is much less common. Recommend you send a request through MyPers to the Assignments folks, assuming somebody at Assignments is slightly more competent than a brain-dead monkey.
-
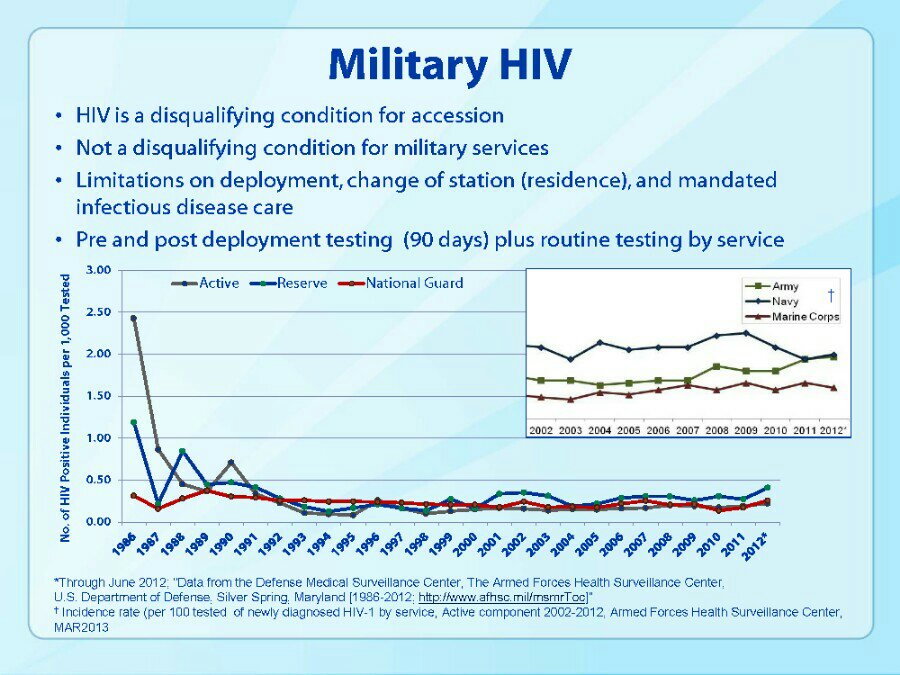
Yep. Doesn't matter. If you've ever broken your nose or had any facial surgery, include it in your history and leave it at that.Though you may be heavily tempted to lie about your medical history to improve your short term chances to join, you would be risking a great deal, especially if you require significant medical evaluation or care in the future. Be honest with your recruiter and all medical personnel. According to the AF Waiver Guide, IBS is defined using the "Rome III diagnostic criteria," which states: At the most basic, it is characterized as "abdominal discomfort or pain associated with disturbed defecation." Therefore, various doctors may over- or under-diagnose IBS, or may use it as a place-holder while they continue to find the actual diagnosis. Further, doctors may diagnose IBS when they are never actually able to to find the cause of particular symptoms, but a definitive coding of IBS looks better in medical records for insurance agencies instead of something non-descriptive like "Abdominal pain unspecified site." The first step is to gather all medical documentation of your evaluations relevant to your condition, particularly visits to any Gastroenterologists (GI). If you haven't been seen by a GI or your PCM for this condition, it wouldn't hurt to be seen again to be able to provide recent documentation. If seeing a specialist would be expensive or difficult for you, you could delay it until after you submit everything to MEPS or MTF via DODMERB (or whoever the Medical Authority will be). Next is whether you will be eligible to join. DODI 6130.03, para. E4.13.c.6. states: Then is the standard for flying duty in the Medical Standards Directory, which states: If you don't meet that standard, unfortunately there is no waiver potential for an IFC I (meaning an applicant/untrained noob). Waivers are only possible for FC II (meaning trained personnel already in the AFSC). In short, assuming your story is accurate, I'd guess you have a 90% chance of clearance. Of course patients often lie and some Docs are sticklers.I've been seeing this as a unit policy, not a standard from any personnelist. It generally looks like (NC)OIC's are trying to manage their manpower with the mission and prevent people from leaving within 30 days of notification. Can anybody verify that all leave, including terminal, needs Commander approval?Please read through the numerous other posts on the board that explain the standard.After your cheating scandal.Attached is a slide from this briefing: https://www.cdc.gov/std/treatment/2010/Military-Webinar-slides.pdf This shows the percentage of NEW cases every year. It doesn't include the AF numbers, but we're about the same as everyone else. Total percentage of all personnel in the US Military is around 0.25%--the exact rate frequently fluctuates due to separations, retirements, and new cases. In contrast, the US general population is between 0.3-0.5%, depending on the estimate (about 1 in 6 personnel with HIV don't know they are positive, so the numbers are fuzzy). Further, the US prison population has the highest incidence, at around 2%. Know that Men who have Sex with Men (MSM, yes that is the official term) are about 2% of the total US population. This statistic is only founded in the behavior of the population, not whether they self-identify as Homosexual, Heterosexual, or Bisexual. However, that 2% account for about 62% of all new HIV cases annually. Intravenous Drug Users (IDU, people that might share needles for illegal substances) account for about 5% of all new HIV cases, but are only around 0.5% of the total US population. That means the remaining 33% of all new HIV cases are contracted by the rest of the population, that is persons that are not IDU's and heterosexual or Women who have Sex with Women (WSW). It is unknown how closely this translates to the US military population, as homosexuality has not been openly allowed in the US military for very long. Also, the reporting and tracking of such detailed demographics differs by the individual state Public Health agencies. The US military obviously reports and tracks all transmittable diseases, but they don't include these behavioral data points. So what should you do? In order: Do not use illegal intravenous drugs and/or share needles Enter a long-term monogamous relationship, especially for MSM Use male condoms (or another barrier device) whenever you have sexual contact Limit your sexual partners to very few people.
 what is your question?You can watch it or read the transcript at: https://www.cbsnews.com/news/whos-minding-the-nuclear-weaponsFor HIV, there is no way around this--your Commander and many people in the Medical Group will know about this. Your command shouldn't allow it to affect your career beyond normal ALC standards. Anybody with passing access to your medical records will know you have it. Medical Personnel really don't care, as a given base has a dozen or more HIV cases. For anything less than HIV, almost nobody in medical gives a damn beyond the mandatory paperwork that gets buried in your record along with everything else. Again, anybody could find it, but who cares? Conceivably, your Commander could coordinate an understanding with the SGH or another high level MDG officer to forward any positive STD findings, however that would be an extreme or unique instance, likely beyond the scope of military necessity, but I've never seen that stop the flow of information to the Commander or any future questioning/investigation. Realistically, this sounds like the paranoid delusion of somebody that doesn't trust their command and is looking for an excuse for a recent shitty assignment. It doesn't add up.see attached.
what is your question?You can watch it or read the transcript at: https://www.cbsnews.com/news/whos-minding-the-nuclear-weaponsFor HIV, there is no way around this--your Commander and many people in the Medical Group will know about this. Your command shouldn't allow it to affect your career beyond normal ALC standards. Anybody with passing access to your medical records will know you have it. Medical Personnel really don't care, as a given base has a dozen or more HIV cases. For anything less than HIV, almost nobody in medical gives a damn beyond the mandatory paperwork that gets buried in your record along with everything else. Again, anybody could find it, but who cares? Conceivably, your Commander could coordinate an understanding with the SGH or another high level MDG officer to forward any positive STD findings, however that would be an extreme or unique instance, likely beyond the scope of military necessity, but I've never seen that stop the flow of information to the Commander or any future questioning/investigation. Realistically, this sounds like the paranoid delusion of somebody that doesn't trust their command and is looking for an excuse for a recent shitty assignment. It doesn't add up.see attached. Have you previously had any eye or vision surgery (PRK/LASIK/etc.)? Do you have any history of eye injury? Have you seen the documentation from the Specialist and/or MFS and were you diagnosed with other conditions such as conjunctivitis, scleritis, corneal opacity/cataract? The Optometry folks may not have started the waiver for you until they had the results of your Ophthalmology consult. Get copies of the documentation if you don't already. The waiver guide may not be much help as it only lists conditions that are waiverable. You may have a condition that isn't waiverable, but may be treatable or correctable to the point that you don't need a waiver.Good advice. My current method of updating recall information into my phone is to log-in to gmail contacts at work and typing everything in, which will push updates to my phone.+1 just for the username. Sent from my HTC One X+ using Tapatalk^ This. The review of your medical records is perhaps a bit more thorough than a perusal, but some technicians are more committed to this audit than others. Sent from my HTC One X+ using TapatalkTimeline function on tapatalk I isn't working following the reboot. Sent from my HTC One X+ using TapatalkAll officers should join MOAA; all enlisted should join AFSA. This is an escalating war of money and constituency sizes. Political finance reform is immensely important, but nobody can play with one hand tied behind the back. Until you can vote, vote with your wallet. Sadly, lobbyists usually push more change than writing your congressman. Sent from my HTC One X+ using Tapatalkare you trolling? Multiple senior leaders have speculated the need to cut 25K between now and approx 2019. Sent from my HTC One X+ using Tapatalk
Have you previously had any eye or vision surgery (PRK/LASIK/etc.)? Do you have any history of eye injury? Have you seen the documentation from the Specialist and/or MFS and were you diagnosed with other conditions such as conjunctivitis, scleritis, corneal opacity/cataract? The Optometry folks may not have started the waiver for you until they had the results of your Ophthalmology consult. Get copies of the documentation if you don't already. The waiver guide may not be much help as it only lists conditions that are waiverable. You may have a condition that isn't waiverable, but may be treatable or correctable to the point that you don't need a waiver.Good advice. My current method of updating recall information into my phone is to log-in to gmail contacts at work and typing everything in, which will push updates to my phone.+1 just for the username. Sent from my HTC One X+ using Tapatalk^ This. The review of your medical records is perhaps a bit more thorough than a perusal, but some technicians are more committed to this audit than others. Sent from my HTC One X+ using TapatalkTimeline function on tapatalk I isn't working following the reboot. Sent from my HTC One X+ using TapatalkAll officers should join MOAA; all enlisted should join AFSA. This is an escalating war of money and constituency sizes. Political finance reform is immensely important, but nobody can play with one hand tied behind the back. Until you can vote, vote with your wallet. Sadly, lobbyists usually push more change than writing your congressman. Sent from my HTC One X+ using Tapatalkare you trolling? Multiple senior leaders have speculated the need to cut 25K between now and approx 2019. Sent from my HTC One X+ using Tapatalk