
stuckindayton
Supreme User
-
Joined
-
Last visited
Everything posted by stuckindayton
-
This is hard to answer without more specifics, but agree with Herk- no harm in pursuing your dreams. You are not wasting anyone's time.
-
MP, Refer to the TBI section (linked from the table of contents). Waivers are plentiful with many caveats on severity, timing, etc of TBI. Peruse at your pleasure. Air Force Waiver Guide Compendium.pdf
-
It's entirely possible you are one of the first ones coming through IFC I with ICLs.
-
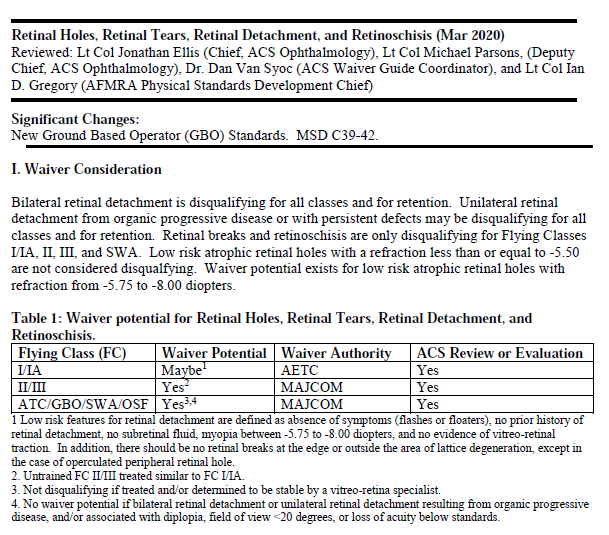
Dank, Assuming you are not a high myope (more than -5.50) and everything is how you describe, there should not be an issue. Waiver guide on retinal holes is below. You are applying for IFC I with a low risk retinal hole treated with retinopexy. According to the first paragraph, your condition might not even be disqualifying, however a history of retinal surgery might dictate an indefinite waiver. Regardless, unless there is something else found you should be GTG. Going through MEPS is always a crapshoot for everyone. IFC I should be better. Cheers, Steve
-
The latest MSD I could find with information regarding this is from 2020. It says "For initial applicants, tympanic perforation or surgery is disqualifying until 120 days post-operative and hearing is normal." It also says "Any conditions that interfere with the auditory or vestibular functions are disqualifying." If you had surgery prior to FCI and it was successful, you would be GTG 120+ days post surgery at your FCI (makes life easy). If you chose not to get the surgery until later, just be careful what you report at FCI as the second statement could come into play and they could DQ you pending surgery. Not a big deal, but could be an administrative headache. Either way works.
-
Anything can be waived if the waiver authority chooses to do so. I'm surprised the WP docs said they'd recommend a waiver since their recommendations are supposed to follow the waiver guide. Things might work differently now. It can't hurt to include IOPs from a civilian doc, but generally the AF doesn't pay much attention to civilian exams for various reasons. I wasn't going to mention what Pbar did, but he is correct. PRK will bring your IOP down. So will eye drops and certain plants that people smoke. I'll just leave it at that. I wish you the best and I'm sorry to not have better feedback. Steve
-
Yea, I'm still lurking around. Eye pressure has been an item that the Air Force has been very wary of historically. A few years ago, the policy was an IOP of 22 or higher was DQing with no waiver. That was plain old stupid because (as you now know), IOP alone really doesn't mean that much unless it is crazy high, ie. >30. Also, IOP is influenced by corneal thickness because the applanation tonometer is simply measuring resistance over an area to determine pressure. Corneal thickness is part of this equation. Thus, thicker corneas tend to read higher and vice versa for thin corneas. Average corneal thickness is around 540 microns. So, the Air Force was willing to give some wiggle room if the corneal was thicker than average and now allows an IOP up to 26 if the corneal is above 540 microns. Personally, I don't like the policy and most of the eye docs at WP don't either. But, the AF doesn't like big changes to policy and getting the corneal thickness measurement in the equation and going up to 26 was a big change and a step in the right direction even if it is not ideal. It sounds like you DO NOT have glaucoma. One of the tests they do called an OCT can demonstrate this. You have ocular hypertension that may lead to glaucoma someday, but that's it. Glaucoma is generally an old person disease. The likelihood of this ever impacting a flying career is exceedingly low. It's a tough one because the AF hears elevated IOP and immediately thinks glaucoma....blindness. The problem is that when you measure something you get a number and when you get a number you need a limit. The docs would prefer the policy just say glaucoma is DQing. That leaves too much room for interpretation and standards don't like that. Best of luck, Steve
-
As I'm sure the docs at WP explained, the concern with a phoria is that it may become symptomatic and result in headaches, blurred vision, double vision, etc. Being tired and hypoxic only adds to this risk. I don't know how they are doing things these days (it sounds like a lot has changed in the five years since I left), but when I was at WP we would do a bunch of tests involved in looking at how well the eyes work together and the amount of effort the person has to exert to overcome their phoria. If we felt comfortable it wasn't going to be an issue years down the road we'd recommend a waiver and vice-versa. Does any of this sound familiar? The fact that you are going to a known airframe that happens to be multi-crew is in your favor since you are not in sole control of the aircraft at all times. Beyond that, I really don't know the waiver climate right now. However, historically, waivers for phorias did happen and it wasn't all that rare. Good luck. Steve
-
Sorry to hear about your friend's misfortune. Gout sucks. The waiver guide states that any history of gout for FCI is not waiverable. It does report that a single FCI waiver was granted at some point, but no specifics are given. I don't know how the civilian world handles it, but my assumption is that there are waivers for gout when it can be managed appropriately. Hate to be the bearer of lousy news, but I wouldn't expect a favorable decision from the Air Force on this one.
-
Google “Air Force MSD” and look at Table One. There are no uncorrected acuity standards for pilot applicants. They were dropped about 5 years ago. Now, there are refractive limits only and they are rather generous. Your corneal scar may or may not need a waiver depending on specifics of the case. You must have vision correctable to 20/20 in each eye at distance and near. They almost never waive that for pilot applicants.
-
MEPS is a complete sham. Laziest POS doctors I’ve ever seen. They don’t care about getting it right. Just collecting a paycheck. You can win this, just keep fighting it. Don’t give up.
-
Thanks O Face and Burt for confirming the path forward. I'm super excited he's flying with the local unit and he just got hired by NetJets as well. FC I is complete, although WP was a bit touch and go. They find stuff even parents didn't know about! This forum is a great resource. Happy I can contribute a little now and then. Cheers. Steve
-
Thank you, will do. Never too early to start learning the ways of the AF.
-
My son got hired to fly C-17s at the local Reserve unit. He was verbally hired in December and they have no idea when he will get picked up for OTS/UPT/SERE, etc. They don't think it will be until next year and he obviously isn't getting paid at this time. However, they want him to swear in next week despite no timetable for moving forward. Is this normal? Is taking the oath akin to signing a contract? Does one incur an obligation when they take the oath or does that only come with signing a contract? I'm confused by the timing of events. Thanks in advance.
-
Pretty much what the optometrist said- the flight doc just needs to confirm you meet all flight standards before you start flying. You don't need to repeat the FC I since it's good for four years, so no worries about whether your prescription is within standard. It's just to confirm that you meet standards for distant/near acuity, depth perception, air puff eye pressure, etc. using either your glasses or contact lenses or both. They will also check your blood pressure, listen to your heart, and all the other good stuff that goes along with a routine exam. In regards to eyes and vision, the primary purpose is mostly to make sure that you have a current set of glasses, especially those highly desirable aircrew specs. No one is expecting a problem at this point.
-
You are correct. Trained pilots are required to meet FC II standards which are significantly more lenient than FC I. If you don’t meet FC II standards waivers are given for most everything at that point. The only time a trained pilot gets DQ’d is when there is a safety of flight concern or when they don’t meet retention standards. There really isn’t an FC II exam comparable to the FC I process. You are required to have an annual PHA, which is done by the flight doc and that’s pretty much it.
-
Annual eye exams are not required for people wearing solely glasses. You are only required to have annual exams if you want to wear contact lenses when you fly for the AF because that requires you to be in the soft contact lens program. If you want to wear them for cosmetic reasons, you don't have to be enrolled in the program, but I suspect you'd have to pay for the contact lens care off base (you typically have to buy your own contact lenses either way). Historically, you had to be in the contact lens program if you chose to wear contact lenses for ANY reason while at UPT, but they changed the policy a couple of years ago to say it was only required if you wore contacts when flying. Correction: The change to the soft contact lens policy from a couple of years ago was to allow trained pilots (and other aircrew) to wear contact lenses off duty without having to enroll in the soft contact lens program. I thought it applied to UPT students, but it does not. If you wear contact lenses off duty during UPT, you are still required to be enrolled in the program and, thus, would be required to have an annual eye exam. Is anyone going to know if you do wear contact lenses on your time? Probably not. The vision check at the flight docs office is basically visual acuity (ie. 20/20 distant and near) and depth perception. You will only be referred to optometry if you don't meet standards with your glasses. I also believe they discontinued annual color vision testing at your annual PHA so that's one less thing to worry about. From what I've heard, glasses work OK at UPT. If you move on to airframes with certain helmet system (JHMCS, JSAM, F-35), contact lenses are often far more practical for compatibility reasons. Spectacles don't fit well under them and are not comfortable at all when wearing the helmets. No worries on the questions. I'm retired. BTW- eye infections are incredibly rare if you don't sleep in your contact lenses and otherwise give your eyes a break from them now and then. Steve
-
Routine eye exams are not required by AF policy. They only time you are required to see the optometrist is if you fail part of the vision screening at the flight doc office or if you wear contact lenses (annual eye exams required). I've heard of some UPT commanders requiring eye exams off all UPT entrants just to catch any underlying vision problems that might impact UPT performance, but that is a one off decision.
-
Your IFC I is good for four years (I believe). Unless you are delayed to such a degree that you won't finish UPT before the four years is up, your refraction is not going to be rechecked during that time. Even if you go in for an eye exam, they won't do the full cycloplegic refraction required to formally measure refractive error. So no worries.
-
I've always assumed the 1 week/month, 6 month follow-up was a requirement for new contact lens wearers. If you are in an approved lens prior to showing up, I would expect the optometrist will enroll you in the soft contact lens program at UPT.
-
-
-
Padre PRK is a non issue in most cases. In fact most people who have a good outcome won’t need a waiver. I wouldn’t worry about it unless you think you have a problem with your eyes/vision. You will need a copy of your pre/post and surgical records for your Flying Class I. The folks at Wright-Patt will take care of everything and should let you know what needs to be done. Best of luck. Let me know if you have any other questions. Steve
-
I don't think there's any way to bypass MEPS. I know someone who recently got hired by a reserve unit and MEPS was the first step. You are correct that MEPS is a crap shoot and can certainly complicate things un-necessarily.
-
SOF_CSO, I'm fairly certain your waivers follow you and don't need to be re-accomplished. AETC is the waiver authority for everyone (active duty, ANG, AFRES) going through UPT so your current waiver should still be valid. They may have expiration dates attached to them which could come into play. Anyone in flight medicine should be able to look them up and find out that information for you if needed. Best of luck.


