aquajam77
Registered User
-
Joined
-
Last visited
-
dude, search function: https://www.flyingsqu...ace-chase-info/
-
-
-
Quite a bit of people outside the engineering hall at his statue last night here at Purdue given that the hall is named after him. Him, Him
-
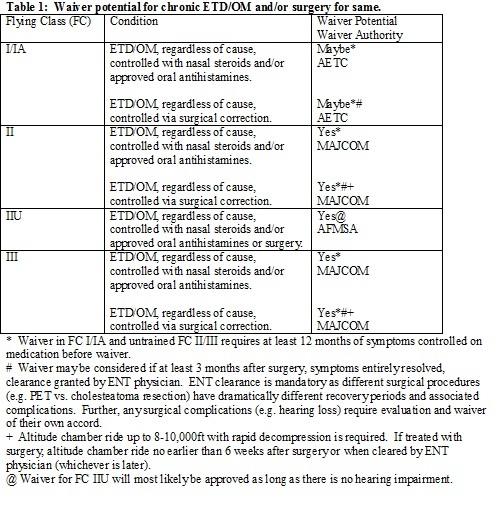
Found the answer to my own question, here it is in case anyone else needs it. Basically you can get tuboplasty to help ear clearing issues and you can get a waiver as long as you are able to then successfully equalize properly (If I read all of this correctly) III. Waiver Considerations. Acute ETD/OM secondary to a transient illness (e.g. viral URI or SAR) requires no waiver but is grounding for flyers until resolution. However, chronic ETD/OM is disqualifying and requires a waiver for FC I/IA, II and III. Also any surgical procedure for correction of ETD/OM is disqualifying for FC I/IA, II and III. It is summarily accurate to emphasize that resolution of ETD/OM and adequacy of ET function are to be assessed on a case by case basis and that no one treatment or procedure, per se, will lead to waiver approval. Regardless of cause or treatment modality, ET functionality must be demonstrable for waiver authority consideration to be granted. In general, the permanent use of PE tubes in flyers is not a good idea, but it is a fact that adults tend to tolerate chronic use of PE tubes better than children. What is important is the operational necessity of using the tubes and the clinical judgment of the flight surgeon and treating otolaryngologist.

-
So apparently this procedure is still (relatively) new, but has anyone heard of eustachian tuboplasty? It's for Eustachian Tube Dysfunction (ETD) and helps to clear out the eustachian tube to be able to equalize the ear better. Does the Air Force have anything on this, whether it's a DQ or not for FC I, II, or III? Thanks
-
pretty interesting... Full Story
-
From personally being 6'7", airline seats are definitely something that are always iffy for me, and definitely a problem for my dad, who is 6'9". Luckily though, I have a longer torso so my legs aren't usually a problem. Whenever we fly, he usually always needs to and is always able to find a seat in the exit row, even if he has to switch seats with someone. Whenever he needs to switch seats the flight attendants are helpful and willing to assist in that process. From never flying Horizon though, maybe that flight attendant was just really pissed at the moment or hates tall people...
-
but aren't F-2s essentially the same as F-16s?
-
Don't know to how "official" official is, but they do exist, and I've seen them at Edwards before as the West Coast Demo Team, part of the 452 AMW. Can't seem to find a good info page on them, but there are pages out there (i.e. March ARB News and Facebook)
-
and now it's even a .gif
-
oh no.... this linky here has ALL of your answers and possibilities with your eyesight Next time Use The Search Function
-
Well I have had rhinoplasty, and just today the removal of the adnoids and reduction of the turbinates. I had rhinoplasty done because my nose was severly deviated, and prevented breathing in both nostrils. When I had the rhinoplasty done, it took me about 6 weeks to fully recover, and since I swim, I was able to get back in during the 5th week. After my surgeon took out the splints (which I do agree must be lodged in the brain) I could definitely breath better, but it still felt like that whenever I breathed through my nose, I was slowly suffocating myself due to the lack of air. 4 months later I checked up with a different ENT who said that my adnoids were extremely large, and that they needed to come out. Not wanting another surgery, I went and got a second opinion, which also said that my adnoids should come out, along with reducing my turbinates. So I finally got that surgery done today, and only 4 hours later, I am feeling fine and I'm well enough to be walking around. Overall, rhinoplasty definitely wins in the pain after surgery category, while my adnoids and turbinates so far just feel slight discomfort, along with the flow of blood that is slowly coming out of my nose right now. I'll inform you more about adnoids/turbinates when I finally fully recover and can provide more of an input
-
you might want to try looking here as it is pinned and has everything on vision... This website is a great resource, but it does help when you use the SEARCH FUNCTION, cuts down on A LOT of redundancy
-
ya, worked for me too, didn't have the huge hassle of trying to stop it