stuckindayton
Supreme User
-
Joined
-
Last visited
Everything posted by stuckindayton
-
It really all comes down to whether you meet the waiver criteria. The flight doc can make any recommendation they choose, but the waiver authority follows the waiver guidelines the vast, vast majority of the time. All of this can be found in the Air Force Waiver guide if you want to review it. I'd post it, but it's a large file. Google "air force waiver guide 2022" and it's your first hit. Best of luck.
-
-
Appreciate the comments. Good to put this old brain to work for something the helps people.
-
Refractive surgery alone is extremely unlikely to result in a DQ. If you have very high myopia, there are other things that could be an issue, mostly related to the retina (lattice degeneration, staphyloma, retinal holes, etc). For applicants, those are generally not waived when related to high myopia even when treated with refractive surgery. Most surgeons would recommend waiting until your eyes have stabilized to get surgery since they will keep changing afterwards. However, the UPT situation puts a unique spin on this. It's not really an elective procedure at that point. That's a discussion you can have with your surgeon. If you are near the true waiverable limit (-10.00 D per my source) then get the surgery ASAP. If you go over -10.00 you most likely aren't going to get a waiver. You can always get PRK/LASIK in ROTC (I believe). The issues with navigating civilian treatment outside of the military don't begin until you enter active duty. Questions are no problem. Ask away. I'm retired, I've got all the time in the world. Steve
-
Trying to get refractive surgery through the military can be a crap shoot. Historically, optometry manning has been a bottleneck and can make it tough to get treated on the Air Force's dime. If you live near a base that has a surgery center (Lackland, USAFA, Andrews, Wright-Patt, Keesler, Travis, JBER, etc), you can typically get it done since the surgery center can do the pre/post op exams. If you are stationed away from those locations, your local optometry clinic may not have the resources to support and if they can't support it, you can't get it done via the military. You can always go the civilian route at your expense, but once you are active duty you must go through the "off base elective medical procedure" process which adds a bunch of hoops which can range from being inconvenient at a minimum and sometimes means you aren't allowed to do it at all. People on flight status have better luck get surgery at military facilities since they are the highest priority, but others may not be so lucky. AF surgery centers are equipped with very good technology and outcomes are excellent. It's just an extremely limited resource. Getting it done on your own ahead of time is certainly the path of least resistance.
-
The cycloplegic is one factor. The other is that the refraction does not push power to give you the best visual acuity (i.e. 20/15 or 20/10). They add power until you can clear the 20/20 line and then stop. That suggests the extra power wasn't necessary. You can still see well when a doc gives you additional lens power, but it's not necessary and can lead to headaches and eye fatigue which is why we try to avoid doing this. Yes, you can get refractive surgery after the FC I. In the past, we would just put the FC I on hold and then submit after the surgery. But, AETC didn't like us doing this so I believe the new process is to submit the FC I as a DQ if you are over -3.00 and then file an addendum after the surgery has been completed and you are successfully recovered and seeing well. I'll check on this and let you know if I'm wrong. I think it's worth pushing forward. Let me know if you have any other questions. I'll check on the process for getting PRK after the FC I if it becomes necessary. Steve
-
Hey Mrs. Zero, I think you understand the situation very well. Not sure I can add a lot, but I'll try. First off, there is no wiggle room over -3.00. Historically, it's been a hard line in the sand. So you are correct, at your current prescription you are not going to be accepted. However, as you also point out, the FCI is done differently than a glasses prescription and is always going to be a little bit lower (at least for near-sighted people). Anywhere from 0.25 to 0.75 lower in most cases. And the docs at Wright-Patt will definitely do anything they can to keep you within standard. I agree with you that the change from 2020 to 2021 is a pretty big jump. Not terribly uncommon with teenagers, but not expected for someone in their 20's or later. Is your vision through glasses from your 2020 exam really lousy? If so, then maybe the change is real. If not, then the extra power probably wasn't necessary. Do not feel bad about applying, even if you are over -3.00. It happens frequently and no one gives you grief about it. You always have the option of PRK/LASIK with only a six month wait after surgery to be re-evaluated. The clock starts on the day of surgery and you have to be six months out on the day of your FC I exam. So, you can get the application started much earlier than six months. Heck, if you are active duty and your commander approves, you can even get the procedure on the AF's dime. Bottom line, go for it. If you get the FC I done and end up over -3.00, you can always get PRK/LASIK afterwards and only have to recomplete a small portion of the eye exam. Best of luck, Steve
-
I hope it works out. Good luck.
-
There's really a couple of things going on that I would have issue with. First, the only measurement of refraction is an autorefraction and that is, frankly, garbage. It's a computer estimate of your prescription and it's often way off. Furthermore, it's not the way we measure refractions for flight physicals. That is based on the doctor's exam, after your eyes are dilated and only to 20/20 (which will always yield a lower prescription) versus to your best vision. Maybe they did that as well, but it's not documented here. If they didn't do that, then you shouldn't be disqualified from FC I per AF policy. Second, how did they test your depth perception? By FC I policy, it must be done with your best correction in place and it must be with glasses. If you don't have glasses that are your best prescription and they didn't make any for you, then that didn't meet FC I policy. So are they going to DQ you from FC I despite not doing the proper tests? I don't know how that works at MEPS. I only saw patients who made it to Wright-Patt. I'd hope they weren't DQing people improperly without giving us the chance to do it right. I know we saw a lot of people who didn't meet refractive standards, but I don't know if they were DQing others and we never saw them. Unless there's more to the story, I'd address the fact that MEPS isn't doing to physical properly to DQ you from an FC I slot. I don't know, maybe that's how MEPS works. But, I was at USAFSAM for almost 20 years and that's not how we did things. Table 4 confuses everybody, myself included when it first came out. It was just an attempt to make PRK and LASIK less restrictive for everybody, but for various reasons they didn't want the limits to be the same for trained aircrew versus applicants, thus we have all sorts of inconsistencies. If you are sure that there's no more documentation, I can ask a few of the admin folks if they run into this and how they handle it. Seems silly to risk losing a C-130 slot over stupidity.
-
Well if your pre-op astigmatism is listed as 3.25 by your surgeon, then you would need a waiver to be FC I qualified, but that won't kick in until you get re-evaluated by the AF. Until then, it's just between you and a LASIK/PRK surgeon if that's the way you choose to go. Happy to help. Keeps my old brain going in these retirement days. Cheers, Steve
-
I'll agree, this is confusing. The pre-op limits of +3.00/-8.00 and 3.00 D of astigmatism were the old limits for everybody- trained aircrew and aircrew applicants. They had been the limits for decades and the AF decided it was time to raise the limits to reflect improvements in technology. So the limits of +3.00/-8.00 and 3.00 D are the limits of what does NOT require a waiver if the outcome is good. Above that, as you see in Table 4 is the "no shit" limits for what the AF will consider for waiver. There are some weird reasons when the hyperopia and astigmatism limits are different for trained versus untrained, but I honestly don't remember them anymore. If you are a civilian applicant, you fall under untrained. Thus, you are allowed to go to those limits. If you are above -8.00/+3.00 and 3 D of astigmatism then you would need a waiver. As long as the procedure is relatively successful you should be fine. The depth perception issue would have to be completely re-evaluated after PRK or LASIK. Note that there is also a 6 month wait time between PRK/LASIK and getting re-evaluated. It's one year for hyperopic (plus) treatments, but I don't think they'd consider your treatment hyperopic since you'd mostly be correcting the astigmatism which is myopic astigmatism. Does that make any sense?
-
Wait, are you currently aircrew for the AF? That creates an odd situation for PRK/LASIK. The limit is 6.00 D pre-op for aircrew applicants, but 3.00 D for current aircrew. If you are AF aircrew, are you AD, ANG, AFRES? If you are civilian aircrew then disregard, the 6.00 D applies. Even if you only wear contact lenses, you still have to get a refraction during your exam. Plus, if you wear contact lenses, the AF policy states that your physical must be done at least two weeks after d/c contact lenses (Note 4 of Table 1 in the MSD).
-
Herk, Congrats on being picked up. The photo you show is your prescription for contact lenses. This will correlate, but will not be exactly the same, as your glasses prescription which is measured during all physicals. I have a couple of questions. Did the optometrist at MEPS do a refraction (i.e. which is better, one or two)? Was it done after dilation? That's what determines where you stand. The equipment used at MEPS, however old, should not change this finding. My best guess is that MEPS probably did it wrong. Just my biased guess. If you can't fight their findings, here are your options: 1. Astigmatism greater than 3.00 is not waiverable for flying class one. It's pretty much a hard line. 2. You could get LASIK or PRK. Untrained aircrew (i.e. applicants) are allowed up to 6.00 Diopters before surgery. That changed someone around 2018/2019 so you might be looking at an older policy. My recommendation is to refute the MEPS exam if they didn't do it exactly like it is specified in policy. After 2 drops of cyclopentolate and only to an acuity of 20/20. See Note 3 of Table One of the Medical Standards Directory. Let me know what you find. Cheers, Steve
-
The test is based around the idea of five stimuli at five contrast levels, but it doesn't always present every stimulus at every level. It uses a staircase algorithm. If you get two stimuli correct at the first (highest) contrast level, it drops down to the third level. If you get two right on that level, it drops down to the fifth (lowest) contrast level. If you get all five right at that level you get a score of 100. If, at any point, you miss a stimulus, it moves back up one contrast level higher (e.g. if you miss one on the third level it bounces back to the second level) and then if you get two more right it bounces back to one level lower in contrast. So although the test is based on a five by five grid, you rarely see all 25 stimuli. Most people see between 9 (the number of stimuli if you never miss anything) and maybe 15 stimuli if you have a mild color deficiency. Of course, this is just for one color for one eye, so multiply that by six (three cones and two eyes) for the complete test. And as I said previously, if your score is near the pass/fail line the entire test repeats for that color to confirm the result. Wright-Patt will almost never repeat the test because: 1) It's already been repeated as part of the computer logic and 2) What score do you take it you fail once and pass once? Like anything in the standards world, it can be very tough to draw the line when someone is on the fence, but it has to be done. I know it sounds a bit like the WP folks might not care (which is absolutely not the case), but they have to process upwards of 50 folks a week and they have limited resources to do so. Difficult decisions have to be made and they are sometimes not what applicants what to hear. But, they will give you every chance to pass that they can. Steve
-
Nate, I believe Wright Patt is still using the Landolt (directional) "C" CCT. There may be a few other clinics out there using the "C", it just depends on who has updated their equipment in the last couple of years. More than likely, your local flight med will have the letter version. In theory, the two should be equivalent. The "C" was introduced to make the stimulus more consistent in difficulty, whereas the letters vary (Z, V are easier, E, F, R, P are harder). However, your score on each test should be similar (within the test-retest variability for each type of device). The version at Wright-Patt (unless they've changed it since I left) will retest you if you score a 50. You effectively have to score below 55 twice to get that as your official result. Once the machine spits out the final result, it's pretty much final. I wouldn't expect them to retest you again at that point. Hope that help. Best of luck, Steve
-
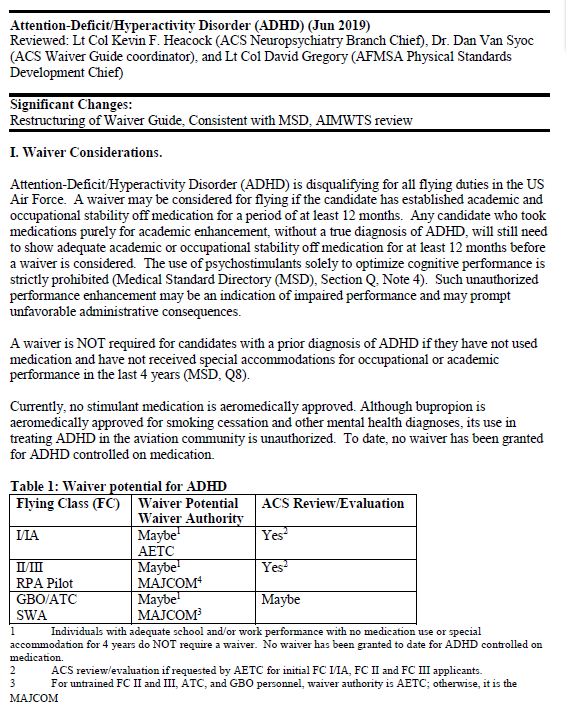
ClearedHot, I'm not a flight doc, but I haven't seen one post on here for a long time so you may not get any other responses. Here's the info you're looking for (From the waiver guide dated 16 Feb 22. Waiver for IFC I is possible. Must demonstrate stability after being off meds for one year prior to FC I exam.
-
Helo, Most of the specifics related to medical have been removed from the AFI and moved to the Medical Standards Directory (attached). The Air Force Waiver Guide (easily Googled) has more information on how medical conditions are dispositioned. Sorry, I don't know have any personal knowledge on the subject. Not my area of expertise. Best of luck. Medical_Standards_Directory.pdf
-
I'm not that kind of doc, but since you didn't get any other replies I'll give you my thoughts. They will certainly review the history and waiver, but I don't think they'll do any more inspection than what everyone else gets. In all my years working at WP I don't recall anyone being sent over to the medical center for a colon scope. Each department is a little different, but for eye folks, our attitude was that if the AF already waived a condition then we were wasting their time giving them our opinion. The only exception was if the waiver was based on incorrect information. Then we would point that out and let them decide how to proceed. Bottom line is that I wouldn't sweat it.
-
-
Agree with both of his statements. Until you are winged, you are untrained. However, I've seen cases where people who had hours in UPT were treated like trained aircrew simple because money had already been invested in them. It's certainly a gray area. You won't get corneal pachymetry annually as the good Capt pointed out, but you will get the air puff. If that reads 22 or above, it will be back to optometry more than likely. But again, if it's been decided your eye pressure is normal for your eye (i.e. given your corneal thickness and lack of evidence of glaucoma) I wouldn't envision it being any issue.
-
Sent a PM.
-
10 exophoria is the standard, but there are some waivers available for people who exceed this. There is not a set limit for what is waiverable. It depends on a number of factors that are determined when the exam is done.
-
Yes, but it's not real common. Having an exophoria is normal, having an extremely large exophoria is a problem.
-
Sorry to potentially state the obvious, but. amblyopia means you have a "lazy" eye. It can mean an eye turn (which would also be labeled as an exotropia), but more correctly it means an eye that can't correct to 20/20. Either an eye turn or not correctable are show stoppers for a pilot slot.
-
Based strictly on the 3.75 value, it is potentially waiverable (and it wouldn't be waiverable for FC I if you weren't to get refractive surgery so in this case if you want a shot, get surgery). Looking at the most recent waiver guide that Google provided me, Table 4 of the "Refractive Surgery" chapter says you can have up to 6.00 D of astigmatism treated with refractive surgery and be POTENTIALLLY eligible for waiver for FC I. There are lots of other factors (is your myopia/hyperopia within limits, is there any ocular pathology that may be causing 3.75 D of astigmatism, is the outcome optimal, etc), but it is POTENTIALLY waiverable. I stress the "potentially" because this was a monumental increase from the previous limit of 3.00 D and when the change was made the understanding among the policy makers was that your post-surgery vision and refractive error would have to be stone cold normal. The waiver guide I'm referencing is a year old so it's not most current guidance, but unless there has been a titanic change in direction, standards aren't getting more strict over time.