Jedi Doc
-
Posts
20 -
Joined
-
Last visited
Recent Profile Visitors
3,032 profile views




Jedi Doc's Achievements
SNAP (1/4)
2
Reputation
-
It is not surprising but disappointing how the public does not understand or appreciate this fact. I hope that aviation's regulating bodies are able to resist the pressure to be reactionary and further limit the current processes in place to treat depressed pilots and then return them to the cockpit. Check out the majority of comments on the previously linked article's FB: https://www.facebook.com/goflightmedicine?ref=tn_tnmn Please share the article so that some may be aware of the unintended consequences of not giving depressed pilots a path to return to flying.
-
The recent Germanwings crash has stirred a lot of discussion on several topics: 1. Importance of having more than one person in cockpit at all times 2. Reporting mechanisms for mental and medical health from all sources of medical care 3. How to address depression and mental health disorders in pilots I have read quite a few blogs and editorials suggesting there is no room for depression or mental health issues in anyone allowed in a cockpit. My personal opinion is that this is the wrong direction to go. There needs to be a way for pilots who are depressed to get back in the cockpit, a pragmatic rational approach is preferred to a 'zero tolerance' one. See recent blog post: https://goflightmedicine.com/germanwings-depression/ What are your thoughts? Should depressed pilots be allowed to fly or get back in the cockpit under certain conditions?
-
The PPP can be entered both by doing UFT and military flight training first or by doing medical school first. I think the former is more common as by becoming a doc first, one typically needs an age waiver (> 30 years old) by the time it's all said and done. I don't know anything about guarantees to return to a specific aircraft. Here is an article written by Lt Col Jay Flottman who is both a flight surgeon and F-15C/F-22 pilot. He describes the entire PPP and his particular route to becoming a PP. https://goflightmedicine.com/usaf-pilot-physician-program/
-
We are still using the AF 1042 where I work. We have been receiving some updates from above with info on the 2992 and the PDF to get feedback. I think this is a great idea as I often see flyers from other services and do not have access to their medical clearance forms. That said, I'm shocked that all 3 branches were actually able to agree on a common form though! If they can do it, maybe even the GOP and Dems can do the same!
-
Yes, the clinical reasoning is the art of medicine and as such there will be some variation in different physicians' assessments. That said, I think most docs can differentiate a normal pattern of upper respiratory and sinus infections from what seems excessive. The big thing you need to do is find a doc who actually cares and realizes the importance to the AF of pushing through a flying class physical. I'd see the flight doc first for the flying class physical and they will make the determination if a referral and/or procedure is required. From what you wrote above, it doesn't sound like it, but I'm not your doc! Just speculating...
-
Pretty broad brush to apply to a large and diverse group of docs. Some people actually do serve because they feel obligated or called to serve in the US military, even if that means personal or professional sacrifice. This doesn't mean these individuals are incompetent or inferior to their civilian counterparts. This makes up at least one category of the higher ranking physicians in the DoD. There are also a large number of senior (and high-ranking) docs who were HIGHLY successful in the civilian sector, but either became unsatisfied or bored in the civilian sector and signed on the dotted line. Anyone that wants to criticize someone who joined the military in their later years and took a pay cut of 50-70% in a medical subspecialty that has a critical need in the military ought to try it themselves. I'm curious what wife's uncle would have to say about AF lawyers?
-
Did you guys put him/her thru the official WSO course or did they just learn from flying and help from the squadron? Why do some heavy pilots feel the need to explicitly mention to me they never actually wanted fighters? ; )
-
WTF is MiCare? Why is the MDG terrible at communication?
Jedi Doc replied to a topic in Aviation Medicine
Definitely the description of a great flight doc. This is the exact reason that flight surgeons are embedded into a particular flying unit. It is crucial to get the aircrew and operators to trust their doc enough to come to him/her with problems knowing that they will do their best to keep them flying, but still always consider safety and the importance of the bigger AF mission. Well said. Well this completely depends on which 'off base care' you're using to compare. The United States lacks a true healthcare system and the quality of care you receive in the civilian setting can vary significantly. There are many clinics and healthcare systems that are considerably weaker and more problematic than the military system, and there obviously exist others that blow military care away. This latter group are the huge tertiary and academic centers that are few and far between (and costs $billions to operate). It's really unfair to compare or expect a tax-funded system like that of the DoD to operate with the same quality as a Johns Hopkins, Cleveland Clinic, or Mayo Clinic. The NY Times attacks on military medicine that continued throughout the summer did exactly this. Used the best healthcare systems as the control and then criticized the military systems for not measuring up. Well that shouldn't be surprising and is hardly a scandal. I have written several blog posts on this topic. Mil med is as you should expect, about as good as most of its civilian counterparts...better than a lot and not as good as many of the largest academic centers. If you want to learn more: A Defense of Military Medicine: https://goflightmedicine.com/military-medicine-defense/ Continued Attacks on Mil Med from NY Times: https://goflightmedicine.com/nyt-mil-med-attack/ Military Health Systems Report Release: https://goflightmedicine.com/mhs-review-report/ -
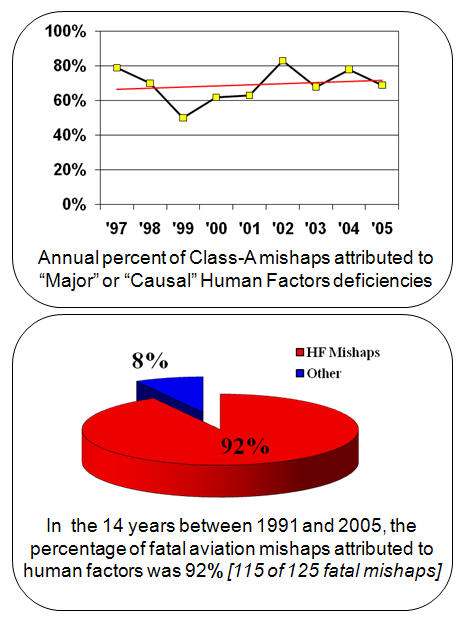
I've been recently reading a lot about the DoD's response to aviation (and other class A) accidents. I read the original book on the Human Factors Analysis and Classification System (HFACS) by the US Navy creators Doc Wiegmann and Shappell. Basically, the book contends: 1. Aviation has gotten super safe, but accidents still happen from time to time. 2. When accidents do happen, they are predominantly caused by human factors (~70-80% of the time). 3. It is important for the safety process and future accident prevention to identify specific human factors and the standardized taxonomy that should be used is the HFACS framework. I completed this research writing a recent blog post: https://goflightmedicine.com/human-factors-analysis/ What do pilot members and investigating officers think about the value of this framework? Useful product or academic dribble?

-
Dead debate is spot on with the reg that concerns you and your 'medical condition' though, it is more of just an anatomic variation. No biggie in the general public, but it could become an issue if your primary duties are being performed in flight. Most of the aeromedical standards really do try to associate the disease/medical condition/anatomic variation with an increased aeromedical risk. Dead debate listed some of the medical standards above. Each one is taken individually though and if you don't meet the standard, an aeromedical waiver must be requested by the appropriate authority. The only medical standard that could concern you is MSD E15: "Deviations of the nasal septum, septal spurs, enlarged turbinates or other obstructions to nasal ventilation which result in clinical symptoms." Unlike all of the standards, this one allows some flexibility because as you see at the end the 'which results in clinical symptoms' allows the doc to make a clinical determination if you need a waiver or not. If I saw you for the flight physical, I would check your past need for medication use, history of sinus infection, ear infections, barotrauma or other recurrent upper respiratory infections/problems. If you didn't have a significantly higher pattern than the general public, you'd likely not require a waiver. Just document the physical finding and go on our way... Each standard also only applies to specific types of IFC physicals. The one above though is a disqualifying condition for all except retention of non-flyers. Hope this make sense!
-
Like any job, you'll have good and bad apples. Aerospace medicine is really a form of occupational med and in order to do the job well, one needs to fully understand the occupational duties of ones particular patients. And obviously the duties vary considerably depending on the aircraft, mission, etc...
-
Well said. Throw a nickel on the grass...
-
Better a lump than a rash I always say. And please no private messages with photos of said rash... Thanks for the advice Deaddebate!
-
There are two common points of confusion with flight surgeons. The first is whether or not a military flight doc is a surgeon as understood by the definition of a particular type of physician who carries privileges to perform invasive surgery. The second is whether or not flight docs are pilots. Many junior enlisted members see the flight doc wearing the same uniform, patches, and rank as a pilot and assumes since they fly, they are also pilots. There is another forum post on the pilot physician program, but this makes up only a very small number of individuals. The majority of flight surgeons are: 1. Not surgeons 2. Not pilots The followup question typically questions why a flight doc has a requirement to fly. I've recently written a blog post on this topic to answer the question (https://goflightmedicine.com/flight-surgeons-fly/), but I really see three primary reasons for flight docs to participate in regular flying duties: 1. To better understand/experience aerospace physiologic stressors 2. To appreciate the particular demands of the aircraft and mission of the assignment flying unit 3. To build trust and social relationships with the flyers Flying is one of the coolest parts about being a flight doc and a required duty since the position was invented during WWI. Occasionally, however, an objection is raised as to if this is really a necessary or even a good idea. I'd be interested to hear the comments from the peanut gallery!
-
Valid point GB!