

stuckindayton
-
Posts
308 -
Joined
-
Last visited
-
Days Won
2
Content Type
Profiles
Forums
Gallery
Blogs
Downloads
Wiki
Everything posted by stuckindayton
-
Yes, that's not 9 esophoria. I forget the conversion, but that number means nothing without converting it. The techs always converted for us so I don't really know what the raw score mean. If you haven't seen one of the docs yet, just hang tight. People failed things all the time and we often could get them through with a little better instruction, etc.
-
9 esophoria is quite a bit. Did you have hyperopic (far-sighted) PRK by chance? It seems unlikely as 99.8% of PRK is for myopia, but esophoria goes hand in hand with hyperopia. Either way, the esophoria could certainly be associated with reduced depth perception (technically stereopsis if you to be technically correct).
-
Yervis, Agree with you 100% on point #1. Regarding point #2, I'm not sure the AF cares that much. Let me give you an example. My son was in ROTC with the intention of becoming an AF pilot (he's since decided the military isn't for him and is going strictly commercial). At the "Welcome to ROTC" ceremony, I asked the ROTC commander if they did any type of medical screening before bringing in young folks whose sole goal was to be a pilot. I cited the example of color vision. About 8-10% of males are color deficient and it's relatively easy to screen. He said they couldn't afford to spend a couple of thousand dollars on the device. One of the first young fellows from my son's class failed color vision at WP and was devastated. Seemed easily avoidable to me. Can't change it (a person's color vision), but would have been a whole lot better to know before spending two or three years working towards an AF pilot slot. I get the whole thing about ROTC being there to create officers, not pilots, but that seems like a bit of a bait and switch to me. As you said, the AF is a bureaucracy. Nothing more. For the most part the individuals who work there are great- some of the best people I've ever met. But, in the end, big blue is there for big blue no matter what anyone says. Don't get me wrong, it can be a great career. I was married into it (i.e. a dependent) for twenty years and spent almost the same amount of time working there myself as a civilian, but in the end the organization's number one goal is self preservation at any cost, even at the expense a lot of good people.
-
Your point is valid. There is no question that some people who would have been perfectly safe bets in hindsight do not get selected and some people who are selected go on to have major medical complications that cut their career short. I'd like to think there was a better way, but short of training everybody and making the final decision based on their UPT performance (which won't happen for financial reasons), I don't know what that better way is.
-
To your question "Does an FAA FC1 translate to military flying duty whatsoever?" Simply put, not really. An FAA medical is based strictly on whether you currently meet the standards for a given class and if you are expected to maintain those standards for some limited length of time (I would assume they are looking for something like 6-12 months of stability since that's how long FAA physicals are typically good for). An AF physical, certainly an initial physical, is based on expected stability of 6-10 years depending on the class. For example, a pilot applicant has a ten year commitment, thus they want someone who will continue to maintain physical standards for that length of time. The FAA AME that is signing your medical doesn't have any vested interest in your flying longevity- only that you meet standards until it's time to renew the certificate The USAF flight doc is employed by the AF to help determine where the AF spends its training dollars. There's no question that getting disqualified sucks. And there was certainly a period of time recently where the AF was extremely short of pilots- and it looks like it's going to happen again soon. But, don't confuse a pilot shortage with a problem finding qualified people to fly. The last year I was at Wright-Patt, we medically qualified more than twice the number of people the AF could train in one year. It's a retention problem, not a recruiting problem. Bottom line is that the pilot selection process is a numbers game. There are people who get lucky and people who get the short end of the stick. I always encourage a person to keep trying and things may eventually work out, but not everyone who wants to fly is going to get that chance.
-
When I was at WP, the policy was that the 20/50 was just used as a benchmark when there was a question about complications after PRK. A person wasn't DQ'd simply because they weren't 20/50. It was to gauge whether a complication (usually scarring after PRK) needed to be addressed. Having said that, the most common reason people aren't 20/50 is that they still have a little residual prescription after PRK/LASIK and the test gets rerun with the correction in place. If you can demonstrate you are capable of 20/50 with correction, that is all that is required. That doesn't drive the requirement to wear correction while flying. That is solely based on the 20/20 and depth perception requirement. The 20/50 is a little bit of a legacy holdover from when PRK had a lot more complication than we see today. Did you also say that you failed depth perception? Is it possible you have a bit of a lazy eye? That would explain both the depth and reduced contrast sensitivity. Perhaps I'm reaching.
-
Change to Air Force Color Vision Policy
stuckindayton replied to stuckindayton's topic in Aviation Medicine
No planned changes to the color test per my ACS sources. There is a push to convert all of the testing to a computerized device called an AVT (Automated Vision Test), but that's still only a discussion and there are no solid plans to do so. -
Change to Air Force Color Vision Policy
stuckindayton replied to stuckindayton's topic in Aviation Medicine
It may be possible. I don't know, but it would surprise me. The two devices agree with each about 98-99% of the time so changing wouldn't affect the pass/fail rate to any meaningful extent. I'll ask the folks at ACS and let you know what I hear. -
Change to Air Force Color Vision Policy
stuckindayton replied to stuckindayton's topic in Aviation Medicine
GHawk, I'm sorry I don't really have an answer. I left Wright-Patt last fall and don't have any privy to recent events. I will say that many of these "exceptions" are based on who is sitting in the decision making seat so they do change with personnel changes. All I do know for sure is that there have been very borderline cases where an applicant was given the thumbs up. -
Technically, for aeromedical purposes, there is no 20/20-. On the OVT (the machine used for visual acuity in flight medicine) there are ten letters on each line (i.e. 20/20, 20/25, 20/30, etc) and you get credit for the smallest line that you get ALL letters correct. Having said that, you are correct that in the optometry world we will denote 20/20- when a person misses a letter on the 20/20 line, or 20/20-2 if they miss two letters. But again, that is not what should be used for a flight physical. It's only the OVT that counts since it's standardized, versus optometry eye charts that may or may not be. They may be improperly calibrated whereas an OVT cannot be adjusted and should always be in calibration. I'm pretty sure this guidance is only found on the Knowledge Exchange, which is CAC protected so I can no longer access it, but I should be able to get it for you if needed. Is there a reason to believe you shouldn't be correctable to 20/20? It's very rare for a young healthy eye to be below this level.
-
Not sure what the question is. Are you asking where it says you must be 20/20 (either with or without correction)? If so, that's in Table One of the MSD (a recent, although maybe not most current version can be found at https://afspecialwarfare.com/files/MSD May 2020 FINAL 13 MAY 2020.pdf). Sorry in advance if I'm missing the intent of the question.
-
Can anyone give recent FC1/MFS Experience?
stuckindayton replied to rotorguy's topic in Aviation Medicine
Depends. Lots of factors. Different docs handle DQ events in different ways. Some will let you know what they've found right away, but others will wait because the entire exam has to be completed and other problems may pop up. Then, they cover everything all at once. Sometimes the doc will base their actions on how they perceive the person is going to take the bad information. It sucks for everyone involved when an examinee is given bad information, takes it hard and then you still have to complete the process. I think it's safe to say that a person will know when something isn't going right, but they may not get the full picture until the end. Speaking for myself, I never wanted to tell someone one thing and then have to retract my statement because of new information. -
Past LASIK- Waiver Required or Not?
stuckindayton replied to TaleMediocre's topic in Aviation Medicine
Don't worry about the timing of the the post-op exams. Those are requirements when current AF flyers get refractive surgery. Not applicable to people who are applying. You are correct, most people don't require a waiver when entering after having LASIK/PRK. Only exceptions are people whose eyesight (i.e. prescription) prior to surgery was crazy high (above -8.00, +3.00 or 3.00 Diopters of astigmatism). There is also a limit for what can be waived (above -10.00, +5.00 and 6.00 Diopters of astigmatism). All this assumes a normal, uncomplicated outcome and that you are at least six months post surgery (12 months for farsighted procedures). You still need (at a minimum) at least one pre-op exam, a surgical report and one post op exam at 3 months or later after the procedure. The folks at Wright-Patt can work with you if you have more specific questions. -
Based on the 2019 aircrew medication list (the most recent I could find, there may be a newer one), minoxidil is not approved due to blood pressure lowering side effects. Finasteride (Propecia) is allowed with a DNiF period required only when first starting the medication to allow for side effects. So, if you're already taking finasteride you should be OK.
-
It was a relatively recent change in policy (maybe two years ago?). CCT done at initial qualification only.


-
Color vision should be one and done at the FC I. But you should get the wonderful puff of air in the eye to make up for it.
-
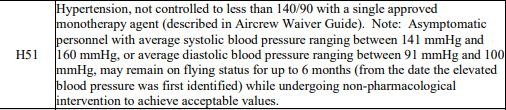
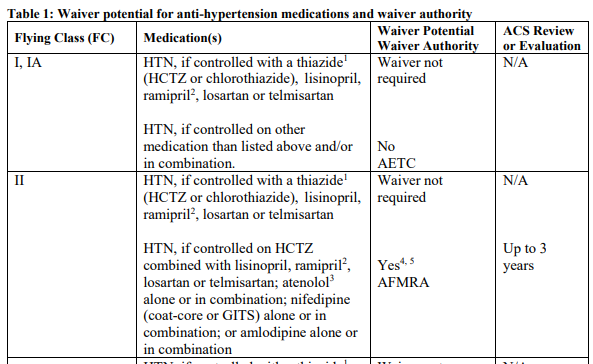
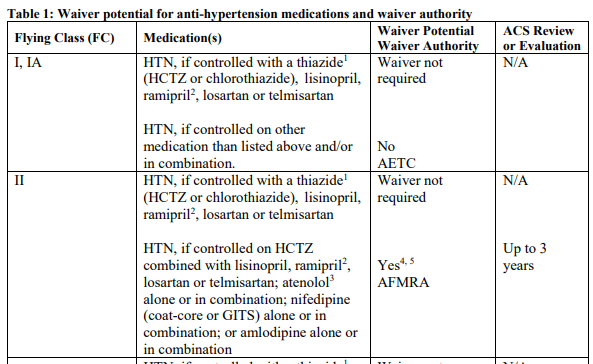
I must caveat my response with the fact that I'm no expert on hypertension and flying. But, according to the most recent Medical Standards Directory I could find (May 2020), here is the standard on hypertension: The most recent waiver guide (April 2020) I could find stated this: Essentially you must must the standard (treated with a single, approved med). Otherwise, there are no waivers for IFC I. Note that these may not be the latest MSD or waiver guide, but nothing changed in the years prior so I highly doubt anything has changed since they were published.
-
Yeet, I'm just an optometrist (i.e. not a real doctor) so forgive me if I'm being ignorant. Do you by chance mean microdiscectomy? If so, I don't have a great answer, but I'll point you in a direction. There is another thread on here that discusses microdiscectomy and my understanding is that it's a no go for any ejection seat, which is mandatory for UPT. Anyway, you may find something useful in that thread. Beyond that, I'm afraid I'm not really of any help. I applaud your attitude about being an officer first. Best of luck.
-
This is, unfortunately, the rule for Wright-Patt. Each refractive surgery center is allowed to determine their "catchment" area and for Wright-Patt it's apparently 100 miles. Since PRK is not a Tricare benefit (it's considered a readiness benefit), then the normal rules don't apply. Hence, WP might be your servicing MTF, but it's apples and oranges when it comes to refractive surgery. Historically, they've had a clinic manager who is pretty set in her ways so chances of sweet talking them into changing their mind isn't good. Off the top of my head, I don't have any really good work-around ideas other than paying out of pocket with a civilian. Its really a bummer since the resources (millions of $$$$ in LASER and other equipment) are literally sitting right there and the cost to the AF to use it is minimal, but their concern is a person who is greater than 100 miles away may be less likely to show up for mandatory follow-ups. FWIW, every AF refractive surgery center has a similar policy, but WP tends to stick by the letter of the law more rigidly than others. Wilford Hall in San Antonio is far more liberal in treating and you might possibly be able to work out a plan with them, but the cost of travelling to SA on your dime probably isn't all that appealing.
-
The expectation is that if there is any way to get the records, even if inconvenient, then they should be obtained. If, however, you make a good faith effort to get them and there are legitimate reasons why that can't happen then there may be some wiggle room. I can't be more specific since it's handled on a case by case basis. Technically medical records are only legally required to be retained by a facility for seven years (in most cases) so this isn't the first time this will have come up.
-
BTW- I didn't notice this the first time around. You're going to have to wait six months from your PRK to complete the IFC I. I would go ahead and get the scheduling going now, but just plan on making sure it's no sooner than six months from surgery.
-
I don't know how much this helps you make the decision regarding the FCI, but consider that if the medical conditions you describe are in your military medical record, they will come to light whether you file for disability or not. The fact that you claim/have disability shouldn't change the decision on your FCI. Those decision should be based solely on the results of your exam. I think someone on this board posted that they received disability for a hearing loss, but passed the FCI hearing test. So, things like that happen.
-
Your FC I will require a trip to Wright-Patt, which your FCIA did not. You'll have to accomplish that. Regarding what specific additional tests will be required is likely going to be up to the docs processing your physical.
-
That's why I was saying my situation was different. I was going traditional IRA to traditional IRA (TSP to Vanguard). I just don't recall TSP caring where my money went as long it was a legitimate investment firm.
-
I may be missing the point here since my situation was a little different, but I moved money from TSP (to a traditional not Roth IRA) when I left the civilian work force and TSP didn't really care who/where it was going as long as I could show I was transferring it to a legitimate investment company (Vanguard). This was one of the few things that was actually easy to do with TSP.


